Abdominal wall hernias
Hernia
The definition of hernia is still under discussion, for practical purposes it is the weakness or protrusion of a structure through an abnormal opening of a layer of the abdominal wall.
Hernia surgery is a procedure that is performed in the United States a million times a year, twenty million hernias are operated annually worldwide, being minimized in many cases without understanding or having a concise understanding of what implies.
For every woman with a hernia, there are twelve men suffering this condition.
Approximatley 85% of hernias from the abdominal wall are inguinal and umbilical hernias.
During the most reproductive stage in a person's life is when up to 50% of abdominal wall hernias appear.
Despite being in the 21st century, there is no perfect surgery, having a discussion of the different surgical techniques and how to solve a problem, which leads to many controversies, explaining the complexity of this pathology.
In most cases the diagnosis can be made with a good Clinical History and Physical examination finding lump, an enlargement of the region, local pain, sometimes they are asymptomatic, needing specialized radiological studies.
Just like a surgical treatment is controversial, there are many classifications for hernias of the abdominal wall.
The abdominal wall hernias may be congenital or acquired.
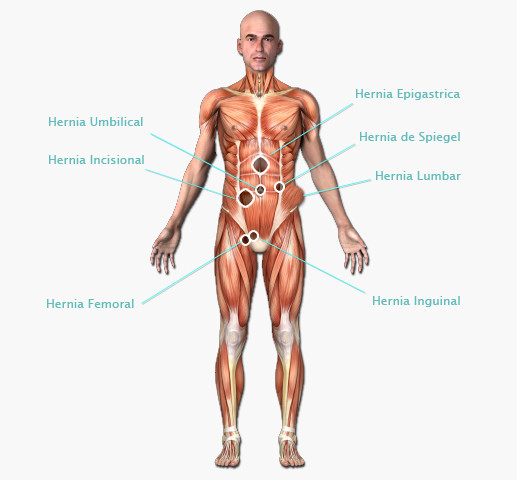
Types of Abdominal Wall Hernias
There is no medical treatment for abdominal wall hernias
The person that presents a hernia is a Chronic Patient, is not just a carrier of an anatomical defect, but a person affected by a problem with a metabolic component that injures the normal structure of the tissues and its healing; specially the patient that presents an incisional hernia.
We must ignore Charlatans who advertise in magazines, newspapers, TV, the use of belts, supports, bands, which are totally inappropriate and should be avoided.
Like in every wall pathology, patients cannot be adapted to one technique, but use de technique needed for each case.
Depending on the Functional-Anatomic constitution of each patient will be the technique use during the surgery, as this is the goal Anatomical and Functional Reconstruction with Normal Tension.
Among the surgical techniques to treat wall hernias, undoubtedly the groin area is where the largest number of techniques and disputes have arisen, using tensional techniques based on tissues and ligaments, anatomical reconstructive techniques, anatomical reconstruction techniques and the placement of prosthesis, open techniques with the placement of prosthesis, endoscopic techniques with placement of prosthesis, and a combination of some of these procedures.
The ideal hernia treatment must be Elective (the patient will choose when, where, how and with whom to be operated).
The late diagnosis becomes critical when there is an incerceration and strangulation (intestine necrosis more often), which is a real emergency.
The delay of a surgical treatment or wasting time, creates a large or Giant Hernia (Hernia with loss of rights home) creating a difficult surgical correction and risk to the patient's life.
In the complexity of these types of problems we should remember RM Kirk's quote "It is not the special method the one that brings good answers, but the enthusiasm for perfection and the ability to achieve it".
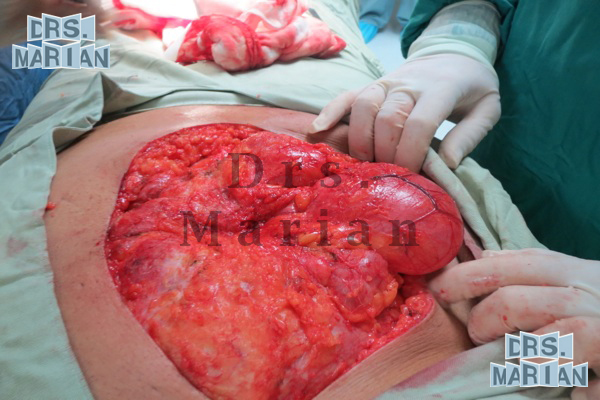
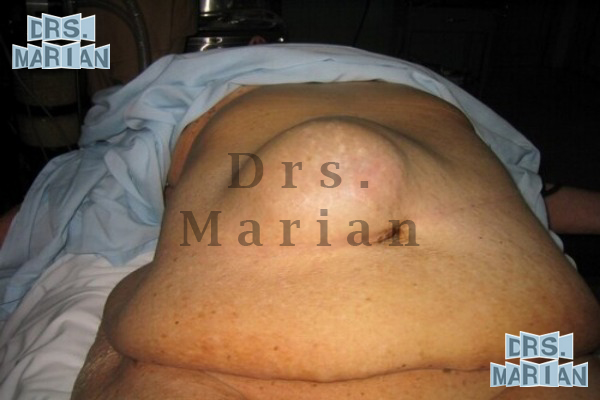
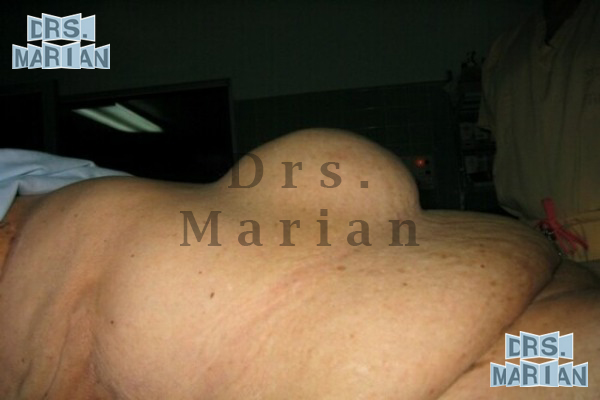
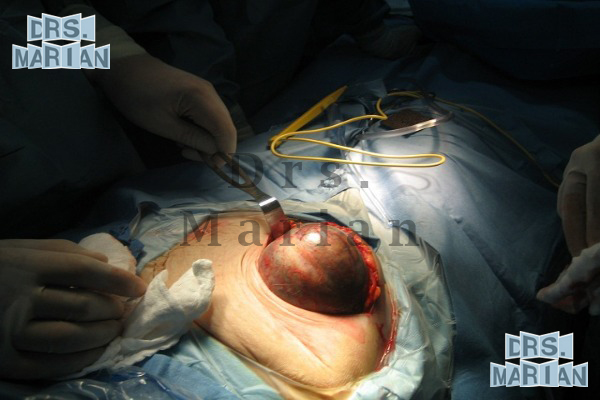
Giant Hernia
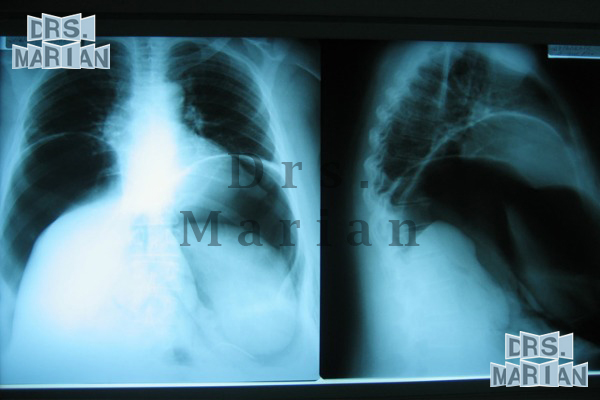
This type of hernia deserves a special mention, since the treatment starts from the preoperative management with the intra-abdominal catheter placement for the creation of a pneumoperitoneum (Introduction of air into the abdominal cavity). Depending on the case, if it were to apply one to two weeks before (there are reports of up to 3 months before) This has several functions, such as the pneumatic dissection of adhesions, the increase in volume of the abdominal cavity to facilitate the reintroduction of the viscera during surgery, in addition to providing the proper voltage for closure of the defect hernial sac.
If the pneumoperitoneum is superior to 3 weeks improves the quality of the response to the scarring, which is very important in this type of surgery
Clinical images of Giant Hernias
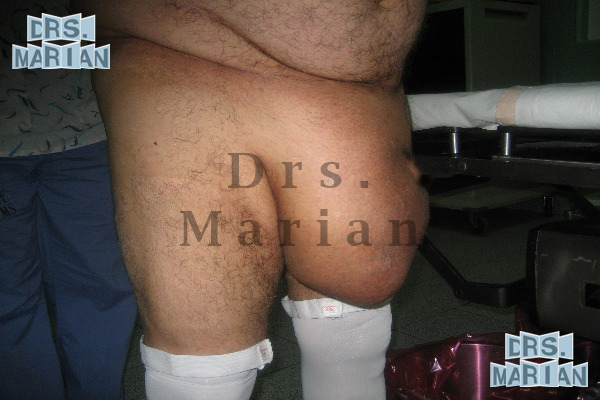
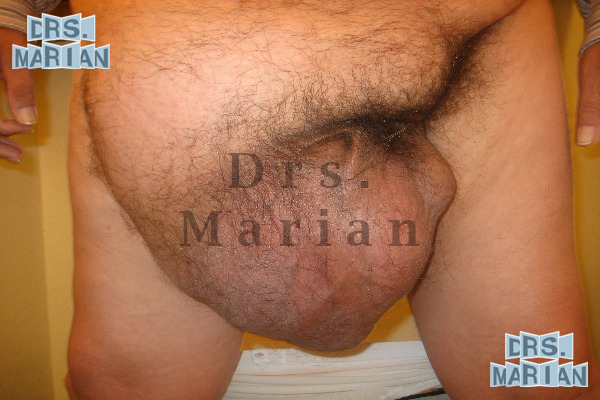
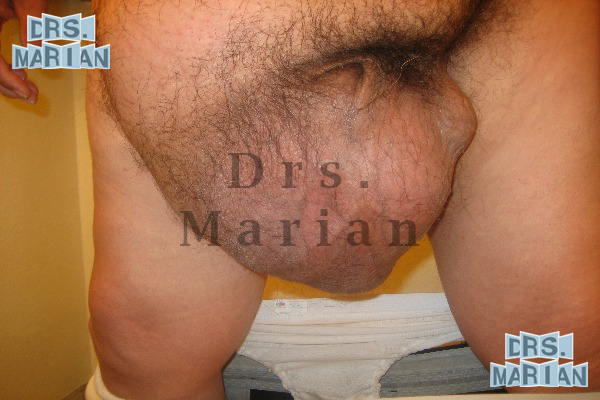
Clinical images of Giant Inguinoscrotal Hernia







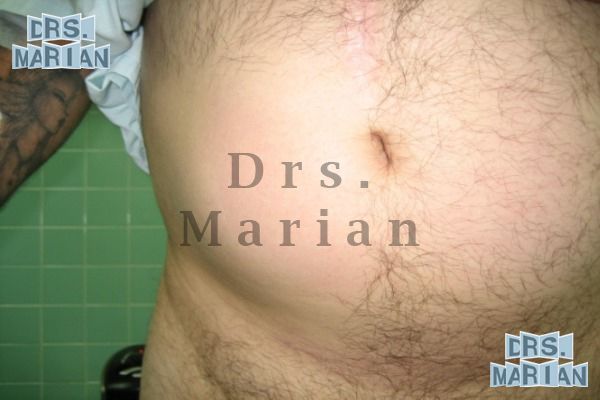
Clinical images of Giant Incisional Hernia
Giant Incisional Hernia: Medical case 1






Hernia Gigante Incisional: Medical case 2




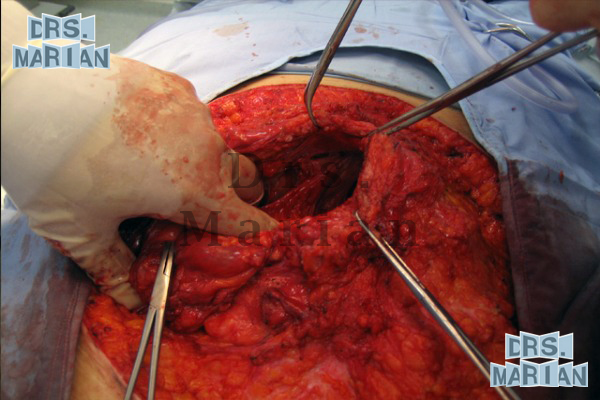
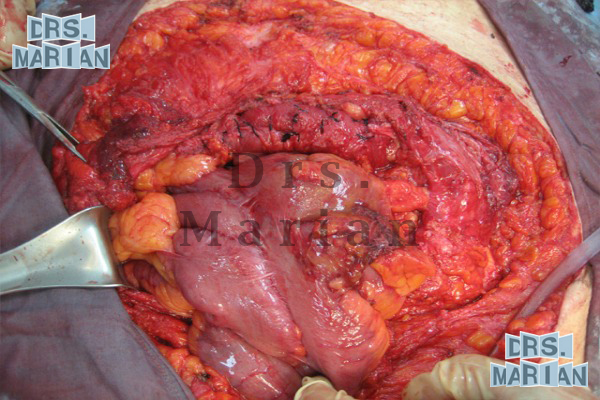


Hernia Gigante Incisional: Medical case 3








Epigastric hernia
It comes in the midline between the navel and the xiphoid appendix, is a protrusion of the preperitoneal fat or peritoneal sac, with or without content, 75% are asymptomatic, studies show that it appears on 10% of the population, it is more common in men 3 to 1; 5% of the hernia's surgery performed correspond to the epigastric hernias.
Clinical images

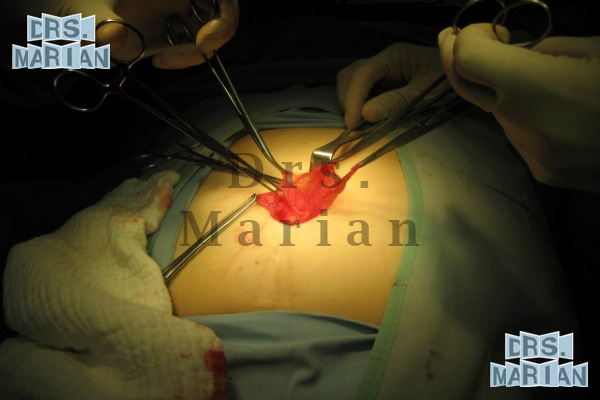
Surgical techniques of the Epigastric hernia
The technique used depends on the size of the hernia defect, its etiology is congenital and anatomic, we will explore the midline by a preperitoneal or subcutaneous dissection, we usually place mesh.
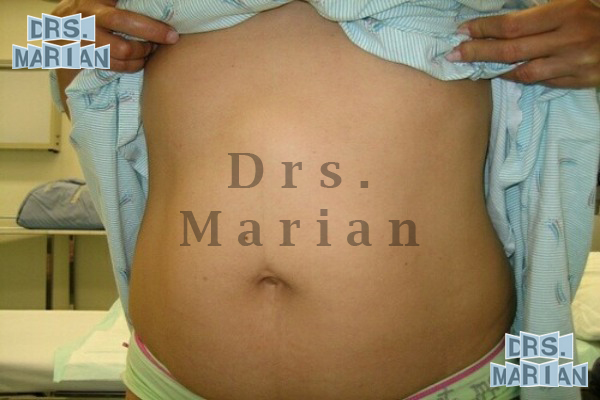
Umbilical hernia
Generally acquired by adults, second place in frequency after Inguinal Hernia, mostly occurs between 25 and 40 years of age, 75% of them appear in women, being the two most important factors, pregnancy and obesity.
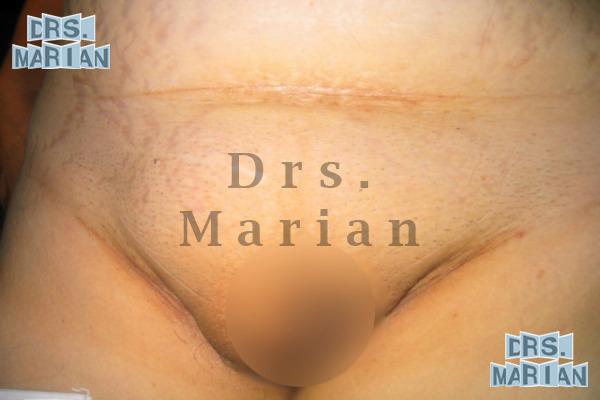
Clinically, it is a mass protruding through or around the navel.
Due to the rigidity of its hernia ring incarceration is common.
Associations between umbilical and epigastric hernias were found, which forces us to perform a scan every time we operate a pathology of the white line (linea alba).
Clinical images







Surgical techniques of the Umbilical hernia
Depending on the size of the hernia defect and the pressure to be carried, will be the technique used, generally a piece of mesh in the preperitoneal plane.
Inguinal hernia
In the adolescent and adult this kind of hernia are acquired, are classified as:
- Direct Inguinal Hernia
- Indirect Inguinal Hernia
- Femoral hernia
- Recurrent Inguinal Hernia
Are the most common abdominal wall hernias and these are indirect inguinal hernias that occupy up to 80 percent.
It is most prevalent in the man in relation of almost 3 to 1 with respect to women.
In women the Femoral hernia approach is the most frequent in approximately 3%, so in the classification of inguinal hernia is the rarest.
Are presented in the most productive phase of the person in the 30 to 60 years of age
There are multiple classifications that there are and surgical techniques have to use what speaks of the complexity of the inguinal canal.
The possibility of recurrence of an inguinal hernia becomes up to a 20% using techniques with tension.
The possibility of recurrence of a hernia already operated is greater with each surgical procedure that is performed.
With the exception of infants, all surgery of inguinal hernias has to fit prosthetic material.
The most common complication is incarceration and more serious is the strangulation of the structures found within the hernial sac; these are surgical emergencies.
Direct Inguinal Hernia
This hernia appears in the mature adult, is more common in women and a less frequently its incarceration, there is a lump at the groin to be amended with different positions.
Clinical images






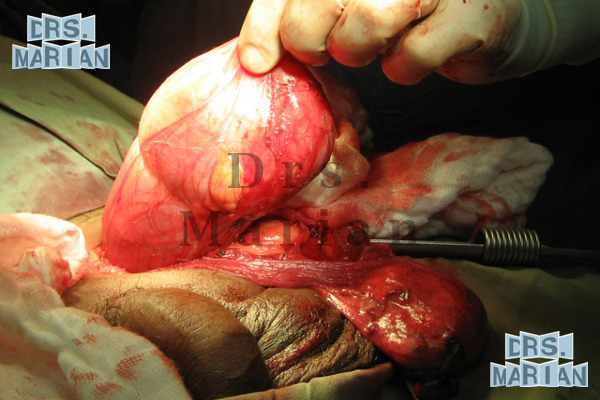
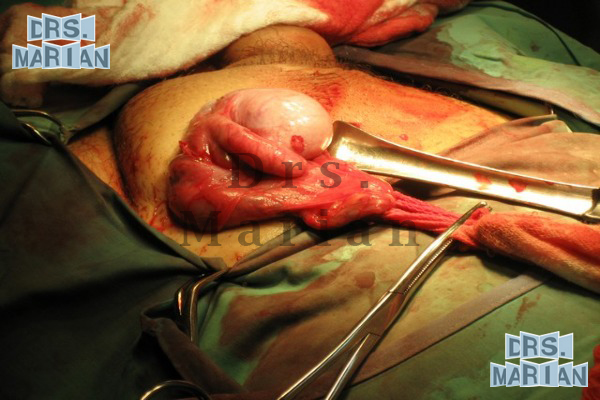
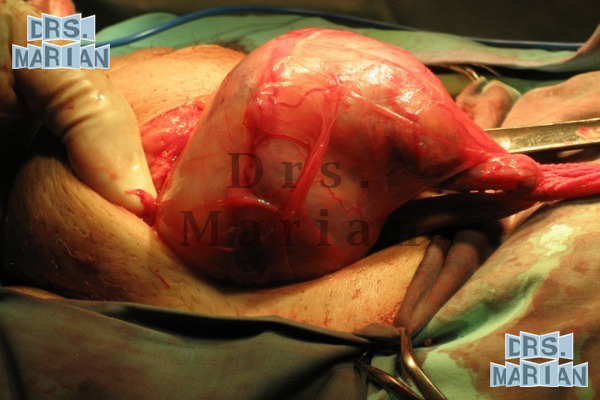
Indirect Inguinal Hernia
It is the most common groin's hernia, with a 70%, is more common in men than women, and more frequent on the right side, due to the contents of the hernia sac and more frequent its incarceration and strangulation due to the journey that follows, is the type of hernia that slips into the scrotum.
Clinical images






Femoral hernia
It is the least common type of groin hernias, and the most difficult to diagnose, more common in females and more prevalent on the right side, patients are able to relate an intermittent pain and in exploration a mass can be appreciated on the inside of the thigh.
Recurrent Inguinal Hernia
Although it has gradually declined over the past few years, there are still these recurrences, which are due to excessive tension in the tissue repair, deficient, hernias that are not diagnosed and were overlooked, or improper technique in the plasty.
The repair of inguinal hernias without placement of mesh and with techniques tension-type headaches have a recurrence by up to 20%
Clinical images



Surgical techniques of the Inguinal hernia
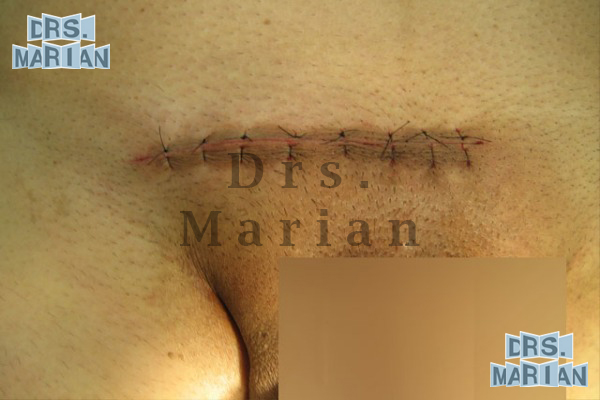
An incision is made approximately from 1.5 to 2.3 inches, in the transverse lower skin fold (at half the distance between the anterior and superior iliac spine and the pubic tubercle).
Depending on the size of the hernia sac, the base is cut or reversed, and instead a PerFix cap is placed, and subsequently mesh reinforcement is placed over the inguinal floor, set with the same material.
The wound is closed with intradermal technique.
Clinical images with Surgical techniques of the Direct and Indirect hernia



Incisional hernia
Performed over 100,000 surgical repairs annually in the United States, third place in frequency of the abdominal wall hernias. Its frequency is bigger in women 3 to 1, due to the larger number of surgeries in relation to men.
Its appearance is the product of a previous surgery, it may arise months or years after the surgery, a protrusion at the intervened area, sometimes with pain.
Is a result of tissues with tension causing disruption in the intervened area.
Factors such as obesity, metabolic diseases, hematoma, infection, malnutrition, contribute to the onset of this condition.
The repair of incisional hernias without the placement of mesh could have a recurrency of up to 50% when the borders are stressed.
Every major hernia defect grater than 5 centimeters should be repaired with mesh.
Clinical images




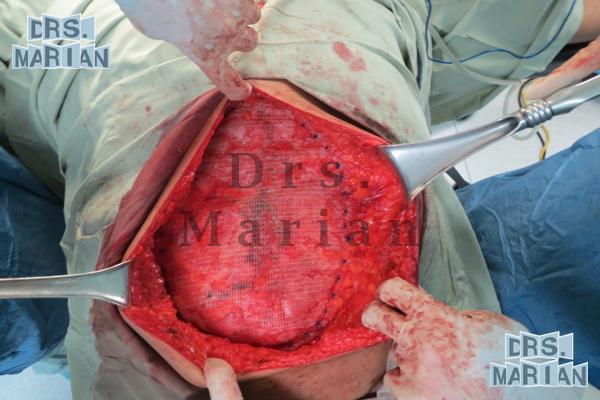
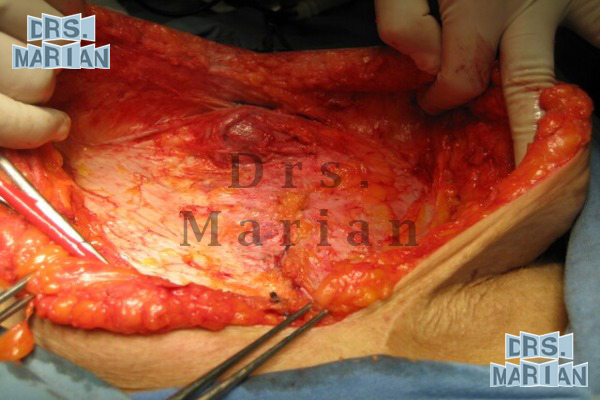
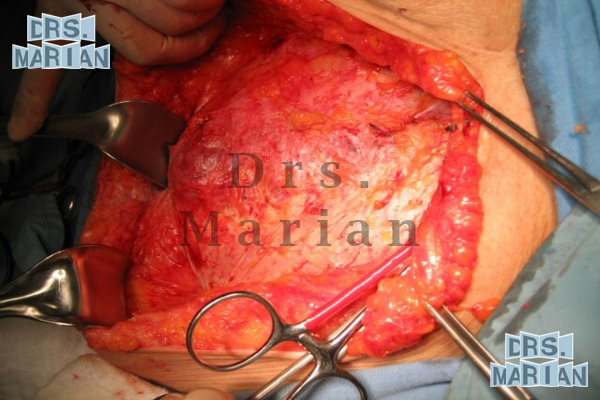
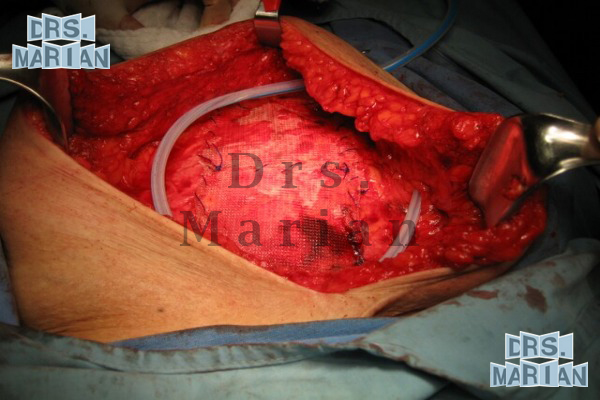
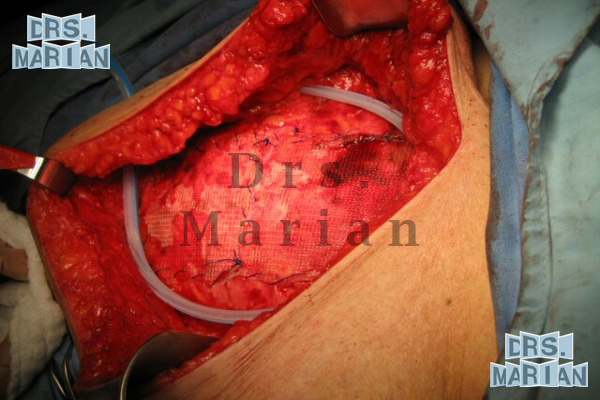
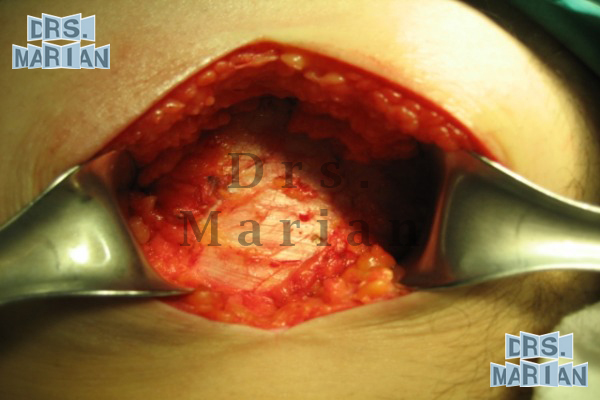
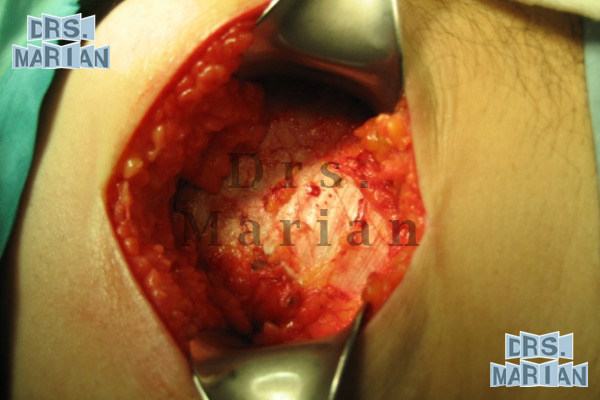
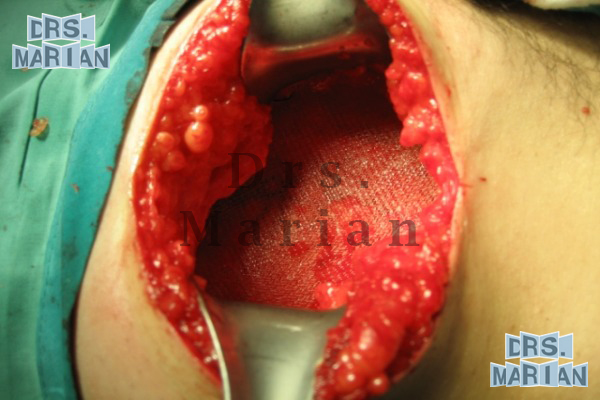
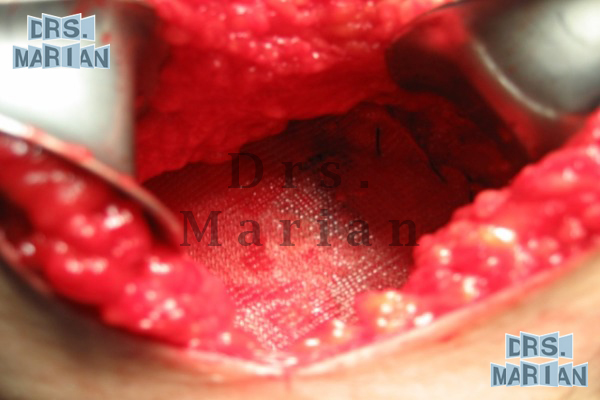
Surgical techniques of the Incisional hernia
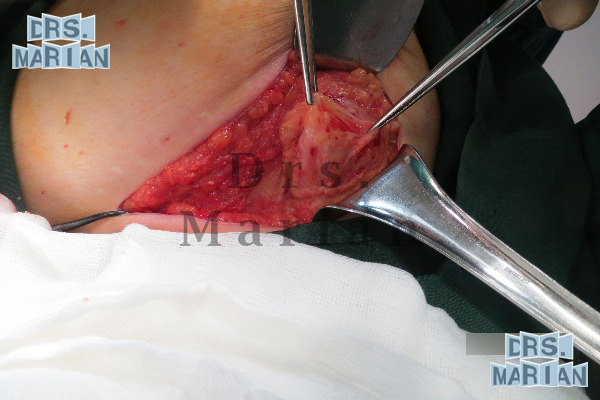
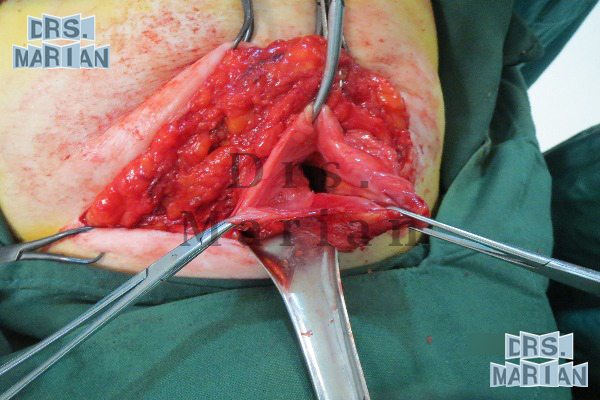
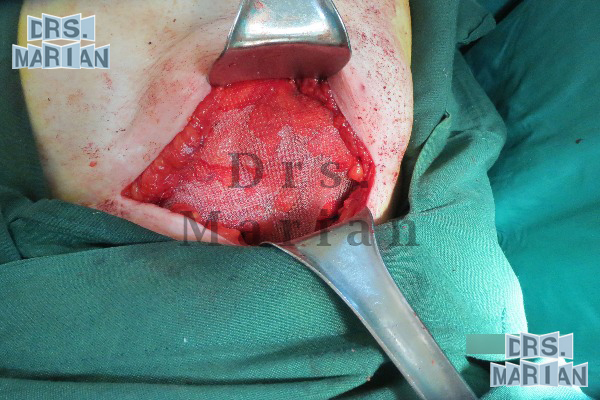
Depends on the location, size and anatomical elements involved, it is usually a muscular and wall reconstruction that will give us a visceral protection, placing mesh fixed to a firm structure, free of tension at a distance of 1.2 to 2 inches to the edge of the hernial ring with no wrinkles or creases, it may require the application of a subcutaneous closed drainage.
Clinical images with Surgical techniques of the Incisional hernia

Spigelian hernia
Make up to 2% of abdominal wall hernias; can be congenital or acquired, there have been reported cases from birth to nonagenarians, affects both sexes and on both sides equally. Spigelian's aponeurosis extends from the eighth costal cartilage to the pubis and is the merging of the internal oblique muscle and abdominal transverse, the area were the hernia sac is weakened and protruded, people with this disorder experience pain and a mass in the lateral abdominal wall in the belt area.
Because the size of the hernia's neck is small, up to 30% of these are incarcerated.
Clinical images
 `
`

Surgical techniques of the Spigelian hernia
Since the size of the hernia defect varies between 0.7 and 4 inches, reconstruction is usually performed, if the defect is small and the muscle is not atrophied, it is sutured in the direction of its fibers, if the defect is bigger, it will be repaired and we will place mesh.
Clinical images with Surgical techniques of the Spigelian hernia

Lumbar hernia
This kind of hernias represent 2% of all hernias, it is the least common of all ventrolateral hernias.
The hernia's area of the lumbar region is limited from above with the twelfth rib, from below the iliac crest, the posterior limit is the outer edge of the spinal muscles and the front by the free end of twelfth rib.
This kind of hernia the 50% incisional or are 1% of all hernias of the abdominal wall, usually presented by renoureterales surgeries or reoperation to repair the hernia by the same urologist.
One of the causes for the formation of this hernia, is that the muscles do not have a strong aponeurosis and the sutures and tissues are torn at the start of the patient ambulation, increasing the problem with the number of reoperations.
Surgical techniques of the Lumbar hernia
A lumbar incision is made, mesh is fixed on the floor of the hernia defect; given that one of the limits is a inexistent bone structure and the others are congenital anatomic faults.
Clinical images with Surgical techniques of the Lumbar Hernia